專注于新型裝飾材料多年,産品以中高端爲主,與國内有名門企合作,是您的信心之選
生産、制造、銷售爲一體的企業,爲您提供更直接的消費

設備良好,配套設施齊全,科技力量雄厚
在增強産品輕度的同時,大幅提升産品質量



從材料上嚴格把控,均選用高質量環保材質
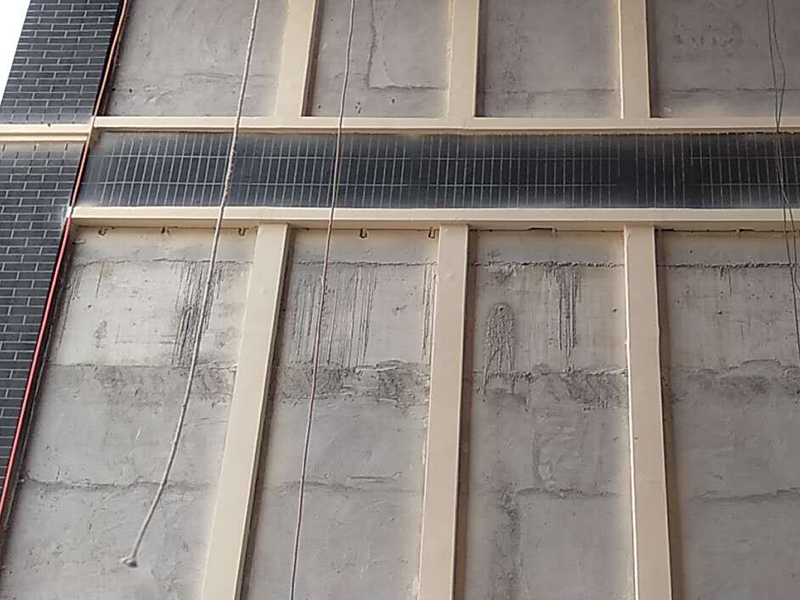
低碳環保施工,讓您遠離霧霾的侵害承接外牆适用于各類建築風格,結構精密,質感細膩
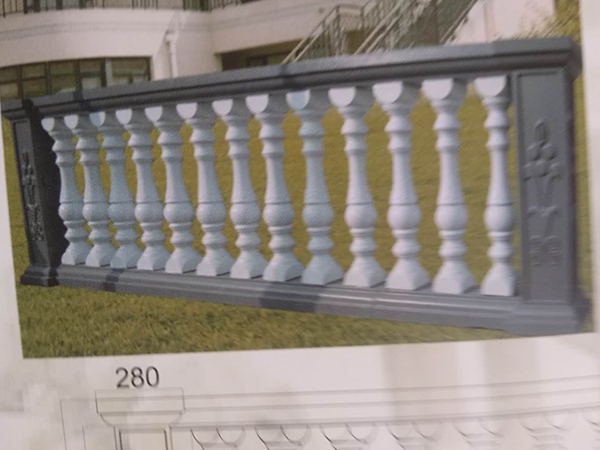
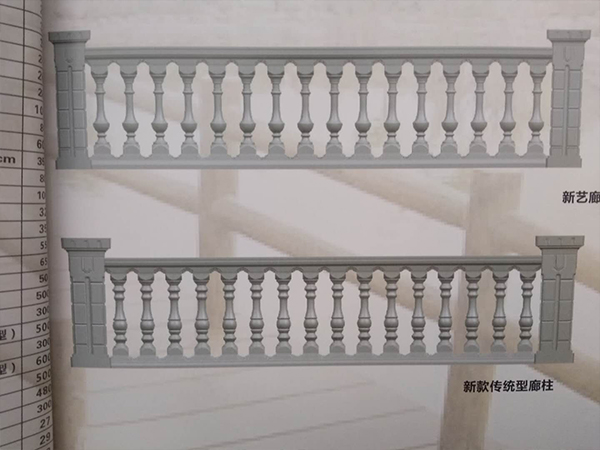
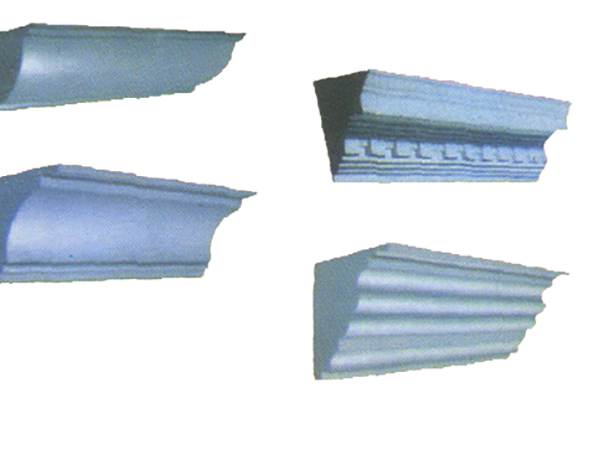
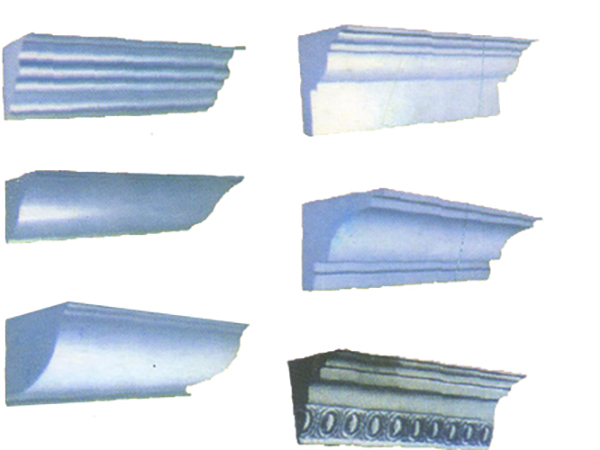
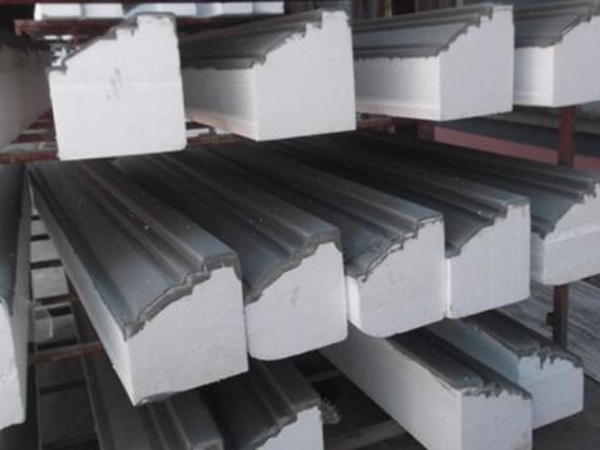
新鄉市騰馬裝飾材料有限公司是一家從事歐式建築設計施工爲一體的現代化生産企業,公司業務涵蓋:EPS構件及EPS線條、GRC構件、羅馬柱、寶平柱、河道欄杆、河堤護欄等房屋外牆裝飾及河道整治産品,客戶可來圖紙加工,産品廣泛應用于大酒店、茶樓、家庭、庭園、别墅及整治工程,我們得宗旨就是誠信管理、科學高效的管理爲基礎,以不斷的科技創新爲動力。堅持以顧客滿意爲中心,爲建設裝飾設計施工和現代化建設做出巨大貢獻,成爲豫北地區客戶信任的企業,爲推動社會新型建築的發展貢獻力量,歡迎各界朋友來我公司參觀、考察、指導并洽談業務。 手機:15560271033 王經理 固話:0373-5618887
了解更多